Global leader in endoscopic weight loss, Triple-board-certified in obesity
If you’re comparing duodenal switch vs gastric sleeve, you’re likely trying to understand which weight loss surgery options actually fits your health goals. Both surgeries can produce significant weight loss, but they work in very different ways and come with long-term commitments.
Because both weight loss surgery options permanently alter the digestive system, understanding the differences matters.
In this guide, we’ll walk through gastric sleeve vs duodenal switch, including results, risks, recovery, and we’ll also cover a third option that you might not know exists.
How Each Procedure Works
The single most important difference in duodenal switch surgery vs gastric sleeve:
The gastric sleeve is restrictive only. Duodenal switch is both restrictive and malabsorptive. That distinction shapes everything — how much weight you lose, what complications are possible, and what your life looks like long-term.
Feature
Gastric Sleeve (VSG)
Duodenal Switch (BPD-DS)
Mechanism
Restrictive only
Restrictive + malabsorptive
Avg. %TWL
20–30%
30–40%+
Hospital stay
1–2 nights
2–3 nights
Operating time
1–1.5 hours
3–4 hours
Diabetes remission
55–70%
Up to 93%
Nutritional risk
Moderate
High (lifelong supplementation)
Reversible?
No
No
💡 Note: Figures reflect percentage of total body weight lost (%TWL). Excess weight loss figures (%EWL) are typically higher and are more commonly cited in older literature. %TWL is the current clinical standard.
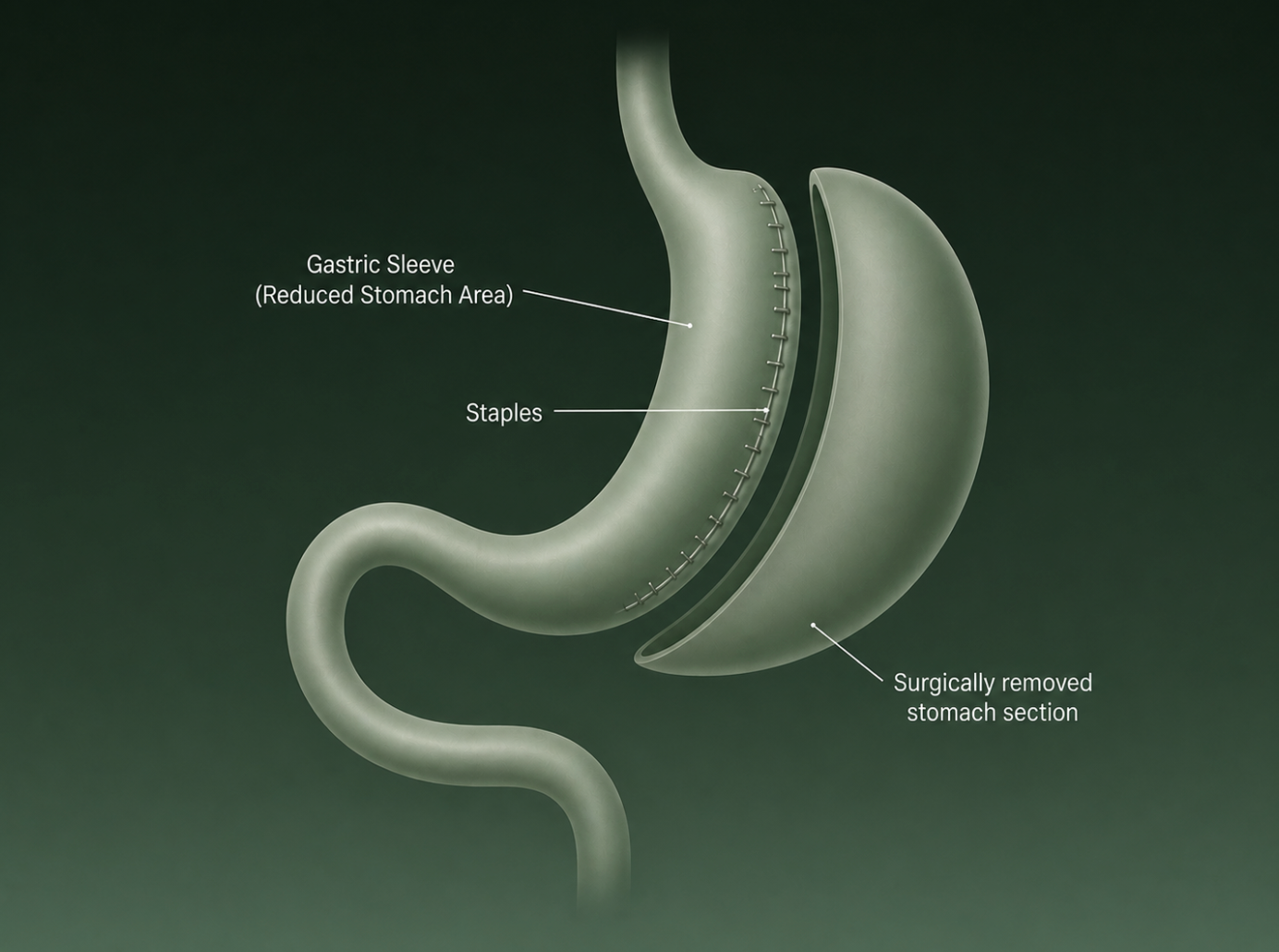
What is gastric sleeve surgery?
Most of the stomach is surgically removed, leaving a narrow sleeve-shaped pouch with no intestinal rerouting.
Alt text: Gastric sleeve (VSG) removes roughly 75–80% of the stomach, leaving a narrow, tube-shaped pouch. You eat less because your stomach holds less. It also reduces ghrelin, the hunger hormone, which helps curb appetite in the months following the procedure. The intestines aren’t touched. That’s what makes it the lower-complexity option.
It’s irreversible. Once the stomach tissue is removed, it can’t be restored.
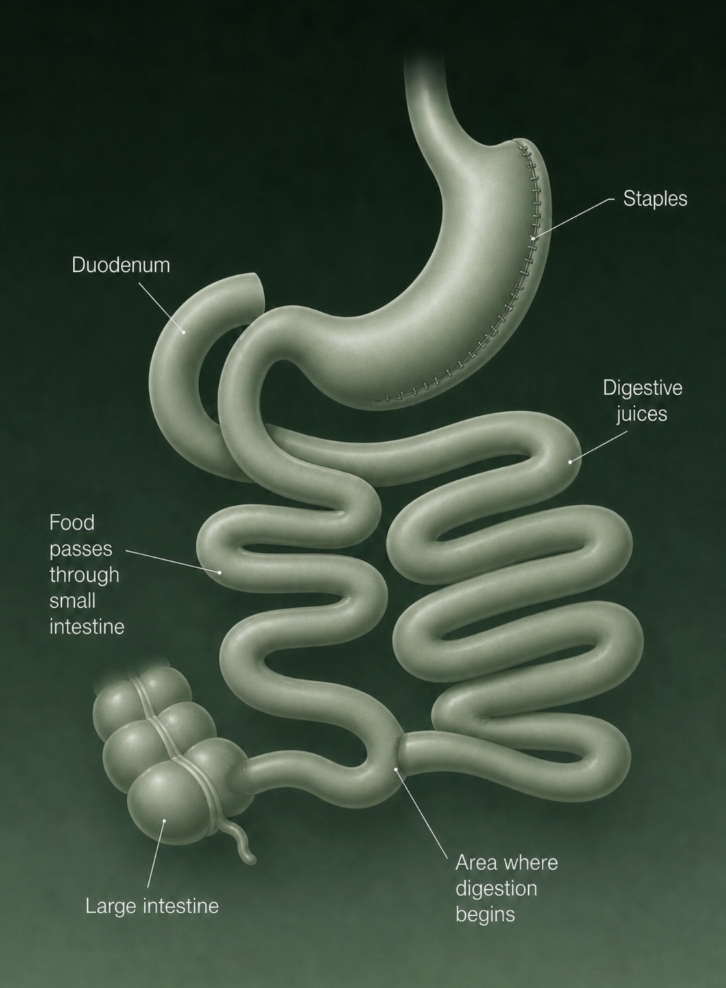
What is duodenal switch surgery?
Combines a gastric sleeve with intestinal rerouting, where food bypasses most of the small intestine, delaying where digestion begins and significantly reducing calorie absorption.
Duodenal switch (DS) combines a sleeve gastrectomy with intestinal bypass. The first part restricts how much you eat. The second part reroutes the small intestine so your body absorbs fewer calories from what you do eat. That dual mechanism is why DS produces more weight loss and more nutritional risk.
One important distinction: DS preserves the pylorus, the valve between the stomach and small intestine. This matters for digestion and is what separates DS from gastric bypass.
SADI-S (Single Anastomosis Duodeno-Ileal Bypass with Sleeve Gastrectomy) is a newer, simplified single-connection variant of DS that’s gaining traction as a lower-complexity alternative with comparable outcomes in early data.
By reducing the stomach and rerouting the intestine, DS limits both how much you eat and how much your body absorbs.
Who Is Each Procedure Best For?
Both procedures can produce meaningful weight loss, but they tend to be recommended for different patient profiles depending on BMI, metabolic health, and willingness to manage long-term nutritional care. According to clinical guidance published by the National Library of Medicine, the typical candidates for each procedure include:
Ideal candidates for gastric sleeve
Adults with a BMI ≥40, or BMI ≥35 with obesity-related conditions such as type 2 diabetes, hypertension, or sleep apnea.
Patients seeking meaningful weight loss through a technically simpler procedure with lower surgical complexity compared with more extensive bariatric operations.
First-time bariatric surgery candidates who want a procedure that does not involve intestinal rerouting.
Patients who may consider additional treatment later if needed, since sleeve gastrectomy can sometimes be revised to another bariatric procedure in cases of inadequate weight loss or regain.
Because the procedure focuses primarily on reducing stomach size, it generally involves shorter operating times and a more straightforward recovery than procedures that also change nutrient absorption.
Ideal candidates for duodenal switch
Patients with BMI ≥50
Individuals with severe metabolic disease, particularly difficult-to-control type 2 diabetes.
Patients who previously had a gastric sleeve but experienced significant weight regain after gastric sleeve and are considering a revisional procedure.
Individuals willing to commit to lifelong nutritional supplementation, regular laboratory monitoring, and strict dietary follow-up due to the malabsorptive component of the surgery.
Because duodenal switch alters both stomach size and nutrient absorption, it carries a higher nutritional management burden and is generally not recommended as a first-line bariatric option for patients with lower BMI, where the risk–benefit balance may not justify the procedure.
Is There a Non-Surgical Option Worth Considering?
Before we get to the risk and recovery data, this is worth pausing on.
For patients with a BMI between roughly 30 and 45 who are weighing procedures like gastric sleeve or duodenal switch, surgery is not the only path to meaningful weight loss. In recent years, non-surgical endoscopic treatments have emerged as alternatives for people who want significant results without incisions or intestinal rerouting.
ESG Stomach Tightening® is a one-time, least invasive weight loss surgery option that reduces stomach volume by up to 75% using sutures placed through the mouth. No incisions, no general anesthesia and no intestinal rerouting required. The stomach’s natural anatomy stays intact.
It was developed by Dr. Christopher Thompson, co-founder of Everself and Professor of Medicine at Harvard Medical School. At Everself, this technique has been refined over years of clinical practice into a proprietary approach with outcomes tracked at 5+ years.
Key facts:
Average %TWL of 18–20%, with durable long-term results
Under 2% complication rate
2–3 day recovery; most patients return to normal activity quickly
Approved for BMI 30+, making it accessible to patients who don’t qualify for surgical bariatric procedures
📖 Read more: ESG vs gastric sleeve — a direct comparison of outcomes, recovery, and candidacy.
Weight loss results: How do they compare?
Both procedures can produce substantial weight loss, but clinical evidence consistently shows that duodenal switch (DS) tends to produce greater long-term weight reduction than vertical sleeve gastrectomy (VSG). Here’s what the duodenal switch vs gastric sleeve results show across different patient profiles.
Short-term results (first 12–18 months)
Both surgeries lead to rapid weight loss during the first year, but the trajectory of duodenal switch vs gastric sleeve diverges fairly quickly because stomach size is reduced differently in each.
With sleeve gastrectomy, early studies commonly report total weight loss of roughly 20–25% of body weight within the first year after surgery. Most patients hit peak weight loss around the 12-month mark, with weight typically stabilizing afterward., reflecting strong early results from the restrictive effect of the smaller stomach.
With duodenal switch, weight loss tends to progress further over the same period because the procedure also reduces how many calories the body absorbs. Patients often reach around 30–35% total body weight loss within 12–18 months after DS.
Long-term durability (3–15 years)
Long-term evidence continues to show a consistent advantage for DS in patients with very high BMI.
In a randomized clinical trial comparing DS to gastric bypass, both more aggressive procedures than VSG, patients who underwent biliopancreatic diversion with duodenal switch maintained significantly greater total weight loss (about 37.5%) over 13–17 years of follow-up.
For sleeve gastrectomy patients specifically, meaningful weight loss can still be maintained over time. A multicenter follow-up study reported that about 31–33% total weight loss was maintained at 15 years among patients who did not require conversion to another bariatric procedure.
These results show that sleeve gastrectomy can deliver durable outcomes for many patients. However, studies consistently find that more malabsorptive procedures like duodenal switch maintain the greatest long-term weight reduction, particularly for individuals starting with very high BMI.
Impact on metabolic conditions
Beyond weight loss alone, duodenal switch is also known for its strong effect on metabolic disease. DS patients often experience superior metabolic control, including improved blood glucose and cholesterol levels many years after surgery.
This metabolic advantage is one reason DS is sometimes recommended for patients with severe obesity or difficult-to-control type 2 diabetes, although the procedure also carries a higher risk of nutritional deficiencies and requires careful lifelong follow-up.
Risks and complications: The full picture
Weight loss outcomes tell only part of the story, the risk profiles in duodenal switch vs gastric sleeve are dramatically different.
Gastric sleeve risks
Staple line leak occurs in approximately 0.5–1% of cases, but can require surgical intervention when it does
GERD (acid reflux) is more common after VSG than any other bariatric procedure — some patients develop it de novo
Weight regain is a documented concern, particularly after the 2-year mark and for patients experiencing it, understanding gastric sleeve revision requirements early makes future options clearer
Irreversible — there is no restoration of the original stomach
Duodenal switch risks
The more complex the procedure, the greater the potential for complications. DS demands respect from both surgeon and patient.
Nutritional deficiencies are the most significant long-term concern: low vitamins A, D, E, K, B12, iron, and calcium are all documented, requiring lifelong, intensive supplementation and regular blood work
Chronic diarrhea and malabsorption issues affect a portion of patients long-term
Operating time of 3–4 hours means longer anesthesia exposure and greater physiological stress
Hospital readmission rates are higher than VSG
Neither procedure offers an “undo.” Both involve general anesthesia and abdominal incisions. If the surgical risk profile of either procedure gives you pause, it’s worth knowing that non-surgical options have advanced significantly and a procedure like ESG Stomach Tightening® carries a complication rate of around 1%, compared to 12–20% for surgical bariatric procedures.
Recovery: What the first weeks look like
Gastric Sleeve
Duodenal Switch
Hospital stay
1–2 nights
2–3 nights
Return to light activity
2–3 weeks
4–6 weeks
Full dietary transition
4–6 weeks
6–8 weeks
General anesthesia
Yes
Yes
Incisions
Yes
Yes
Reversible
No
No
VSG recovery is shorter, but “shorter” is relative. Most patients are off work for 2–3 weeks and restricted from strenuous activity for 4–6 weeks. DS recovery is longer and more demanding, with a more complex dietary progression.
Both procedures carry the same irreversibility caveat. That’s not a reason to avoid them if they’re right for you — but it is a reason to be certain before you proceed.
Choosing the right procedure for your body
Here’s the honest summary:
Duodenal switch is more powerful, but it’s also more demanding. It’s appropriate for patients with super obesity or severe metabolic disease who can commit to intensive long-term monitoring. It’s not a procedure to choose for convenience or because the weight loss numbers are higher.
Gastric sleeve is simpler, still clinically effective, and works well as a first-line surgical option for patients in the BMI 35–50 range. The risks are real, but they’re lower than DS for most patients.
ESG Stomach Tightening® is a compelling third path for patients in the BMI 30–45 range who want meaningful, durable results without the surgical risk of either procedure. No incisions, no intestinal rerouting, 2–3 day recovery — and outcomes backed by 5+ years of follow-up data.
No procedure is universally best. The right choice is personal, and it depends on your BMI, metabolic health, risk tolerance, and long-term lifestyle capacity. Not sure which path fits your goals?
For patients with super obesity (BMI 50+) or severe, poorly controlled type 2 diabetes, DS generally produces superior weight loss and metabolic outcomes. For patients in the BMI 35–50 range, the higher complication risk and nutritional demands of DS often don’t justify the additional weight loss over VSG. “Better” depends entirely on your starting point and health profile.
Can you convert a gastric sleeve to a duodenal switch?
It’s not appropriate for every patient — candidacy depends on anatomy, overall health, and the time elapsed since the original sleeve, which is why reviewing gastric sleeve to duodenal switch revision criteria carefully matters before pursuing it.
What is SADI-S and how does it differ from a traditional duodenal switch?
SADI-S (Single Anastomosis Duodeno-Ileal Bypass with Sleeve Gastrectomy) is a simplified version of the duodenal switch that requires only one intestinal connection rather than two. Early clinical data suggest comparable weight loss and metabolic outcomes with a shorter operating time and potentially lower complication risk. It’s increasingly offered as an alternative to traditional BPD-DS, particularly at high-volume centers.
What non-surgical weight loss procedures exist as alternatives?
ESG Stomach Tightening® is the most clinically validated non-surgical option for patients in the BMI 30–45 range. It reduces stomach volume endoscopically, with no incisions, no general anesthesia, and a 2–3 day recovery. Gastric balloon therapy is another non-surgical option, typically used as a shorter-term intervention.


.BHfOK2WZ_Z1phpgG.png)

