Duodenal Switch vs. Gastric Bypass: Key Differences Explained
Duodenal switch vs. gastric bypass: which surgery delivers better results? Compare weight loss, risks and why some patients choose a non-surgical path.


Global leader in endoscopic weight loss, Triple-board-certified in obesity
Choosing between bariatric surgeries isn’t a small decision.
You’re probably here because smaller options haven’t worked. That’s not a willpower problem, it’s biology. Duodenal switch and gastric bypass are two of the most aggressive tools we have. They’re also not the only options.
Many patients researching these weight loss surgery options want one thing: clarity on which path actually fits their health goals and risk tolerance.
In this guide, we’ll break down the key differences in duodenal switch vs gastric bypass, including weight loss outcomes, risks, recovery, and who each procedure is best suited for.
What Is the Duodenal Switch?
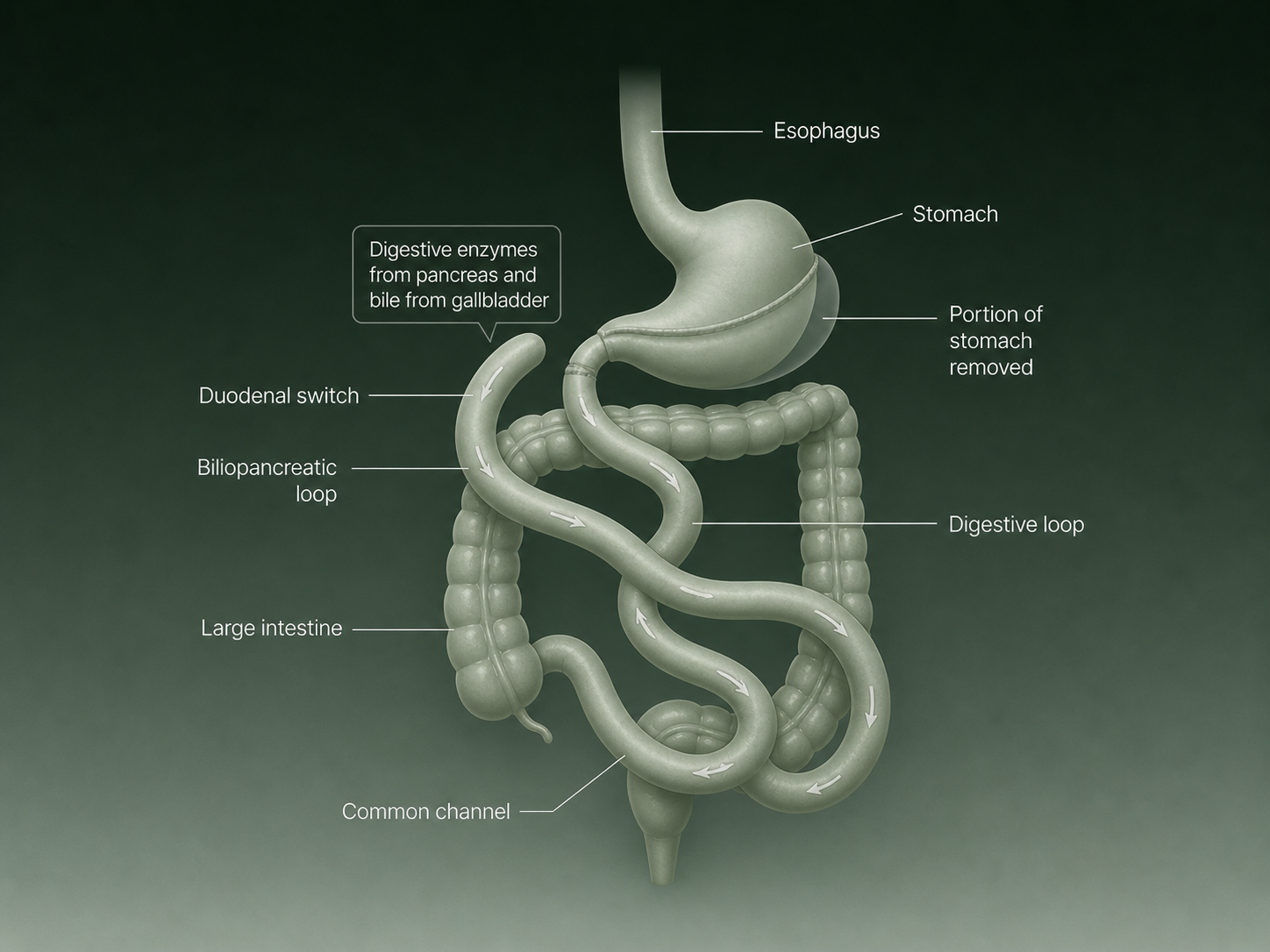
The duodenal switch combines a sleeve gastrectomy with intestinal rerouting, separating the digestive and biliopancreatic loops to maximize both restriction and calorie malabsorption.
The biliopancreatic diversion with duodenal switch (BPD-DS) is one of the most aggressive bariatric procedures available. It combines two mechanisms: restriction (reducing stomach size) and significant malabsorption (rerouting the small intestine to limit how much fat and calories the body absorbs).
Because it works on both fronts, it tends to produce the highest weight loss of any bariatric option — but also carries the most complex risk profile, which is why many patients researching duodenal switch surgery vs gastric bypass spend time weighing the trade-offs.
How the stomach is modified
In the first stage, roughly 70–80% of the stomach is removed along the greater curvature, creating a narrow sleeve-shaped pouch. This reduces food intake by limiting the volume the stomach can hold.
How the intestines are rerouted
The second stage is where the “switch” happens. The small intestine is divided and reconnected so that digestive juices (bile and pancreatic enzymes) meet food much further along the intestinal tract than normal.
This dramatically reduces how much fat, protein, and fat-soluble vitamins the body can absorb, which drives significant weight loss but also raises the risk of long-term nutritional deficiencies.
What Is Gastric Bypass (RYGB)?
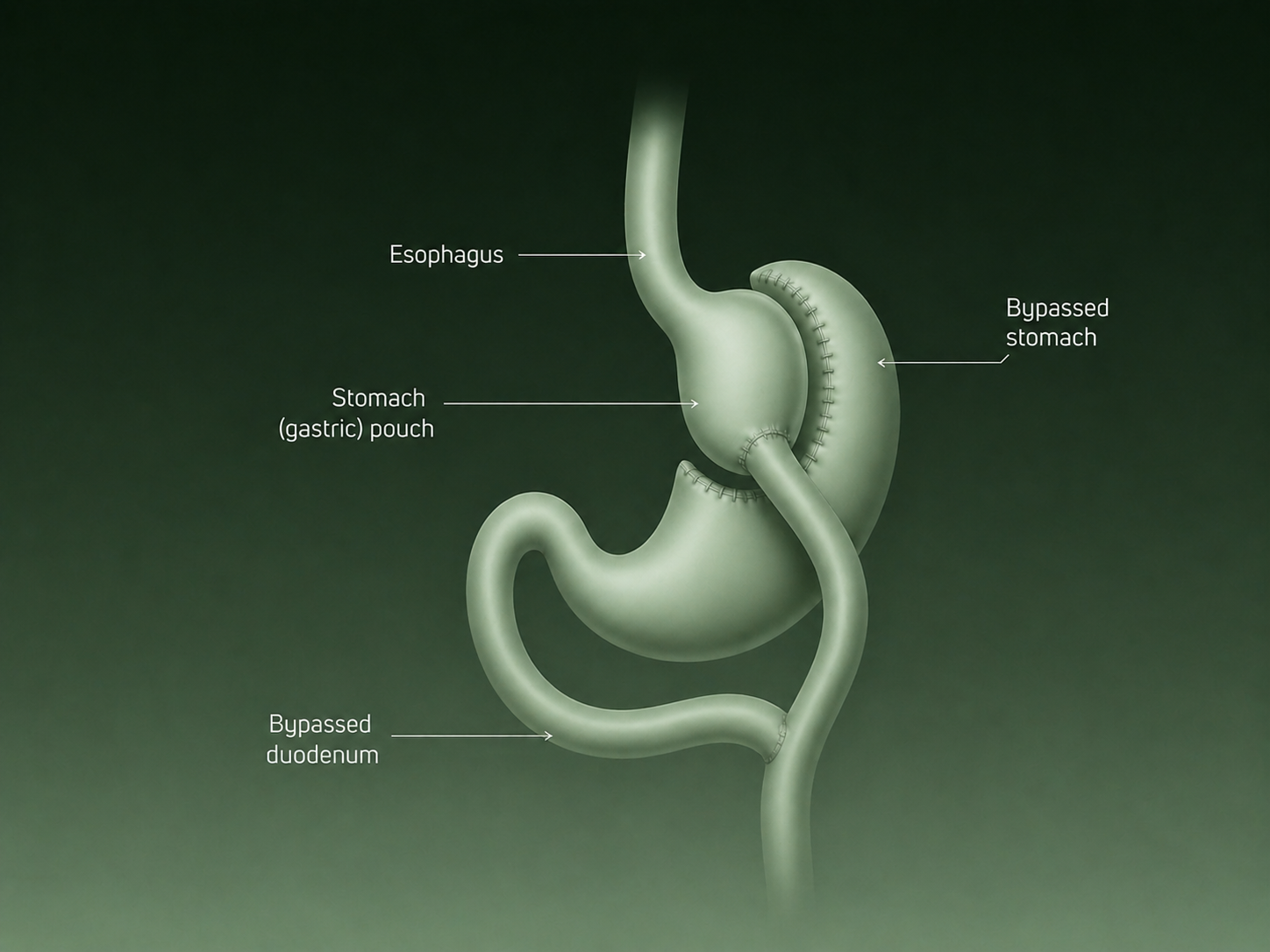
A small gastric pouch connected directly to the small intestine bypasses most of the original stomach and duodenum, reducing both portion size and calorie absorption.
Gastric bypass, medically known as Roux-en-Y gastric bypass (RYGB), is one of the most commonly performed bariatric surgeries for treating obesity. The procedure works through two mechanisms: it reduces the size of the stomach and changes how food moves through the digestive system.
Together, these changes help patients eat smaller portions while also decreasing the number of calories the body absorbs.
Because of its balance between effectiveness and risk, gastric bypass is typically recommended for adults with a BMI of 40 or higher, or BMI 35+ with obesity-related health conditions such as type 2 diabetes, high blood pressure, or sleep apnea.
How the stomach is divided
During gastric bypass surgery, the surgeon separates a small portion of the stomach to create a pouch roughly the size of an egg. This new pouch becomes the patient’s functional stomach.
The remaining, larger portion of the stomach stays in the body but no longer directly receives food. Instead, it continues producing digestive enzymes that later mix with food further down in the digestive tract.
How the intestine is rerouted
After creating the stomach pouch, the surgeon connects it directly to a lower section of the small intestine, bypassing the first part of the intestine where some calorie and nutrient absorption normally occurs.
In discussions around duodenal switch vs roux-en-y, gastric bypass is often considered the more moderate procedure because it balances meaningful weight loss with a lower complication profile.
Who Is a Good Candidate for Each Procedure?
For patients researching duodenal switch vs gastric bypass, BMI range and metabolic health are usually the first factors surgeons evaluate before recommending a specific procedure. Both procedures can deliver meaningful weight loss, but they’re designed for different types of patients.
Here are the key factors doctors consider when recommending each procedure:
Ideal candidates for the duodenal switch
The duodenal switch is typically reserved for patients with a BMI of 50 or higher, or those with a BMI around 40–50 who have severe metabolic conditions like type 2 diabetes that haven’t responded to other interventions. Candidates need to commit to lifelong nutritional management — including regular blood work and daily supplementation — because the malabsorptive component of this procedure is permanent and intensive.
Ideal candidates for gastric bypass
Gastric bypass is generally recommended for patients with a BMI of 40 or higher, or 35 and above with obesity-related health conditions such as type 2 diabetes, hypertension, or sleep apnea. It’s often the preferred choice for patients with significant GERD, since the anatomy change tends to improve reflux.
The duodenal switch, by contrast, can worsen acid reflux in some patients because the sleeve component increases gastric pressure. Patients typically require a lower level of nutritional monitoring than duodenal switch patients, though lifelong supplementation is still necessary.
What if surgery isn’t the right fit?
Both procedures are irreversible, require significant lifestyle adjustment, and carry real surgical risks. For patients with a BMI in the 30–45 range who want meaningful weight loss without permanent anatomical changes, ESG Stomach Tightening® offers a different path entirely.
ESG is one of the least invasive weight loss surgeries. It is a one-time, non-surgical endoscopic procedure that reduces stomach size from the inside using sutures — no incisions, no scars, and no rerouting of the intestine. Recovery typically takes 2–3 days.
Clinical research shows ESG can lead to up to 20% total body weight loss within the first year, with studies reporting 16–20% weight loss sustained over several years. Because the procedure doesn’t bypass the intestine, it avoids the malabsorption risks seen with more aggressive bariatric surgeries.
Duodenal Switch vs. Gastric Bypass: Side-by-Side Comparison
If you’re evaluating duodenal switch vs gastric bypass, the comparison below summarizes how the procedures differ across weight loss, risks, and recovery.
| Metric | Duodenal Switch (BPD-DS) | Gastric Bypass (RYGB) |
|---|---|---|
| Average total weight loss | 35–45% TWL | 25–35% TWL |
| T2 diabetes remission | 90–95% | 50–65% |
| Ideal BMI range | 50+ | 40–50 |
| Hospital stay | 3–5 days | 2–3 days |
| Nutritional deficiency risk | Higher (protein, fat-soluble vitamins) | Moderate (iron, B12, calcium) |
| Complication risk | Higher | Lower |
| Reversibility | No | No |
Weight Loss Results: How Do the Outcomes Compare?
Both the duodenal switch and gastric bypass can lead to significant weight loss, but research consistently shows the duodenal switch produces greater reductions over time.
In one long-term clinical trial, patients with a BMI between 50 and 60 who underwent the duodenal switch lost about 33.9% of their total body weight at 10 years, compared with about 20% after gastric bypass. For patients in a lower BMI range, outcomes for both procedures may differ from these figures.
For patients exploring options that do not involve surgery, it may also help to compare ESG vs gastric sleeve to understand how non-surgical and surgical restriction differ in expected weight loss and recovery. Of course, the procedure itself is only part of the equation, which is why Everself’s 12-month concierge care program pairs every patient with ongoing nutritional and lifestyle support designed to protect results long-term.
Risks and Complications: What You Need to Know
Duodenal switch risks
Because BPD-DS is the most anatomically complex bariatric procedure, it carries the highest complication profile. The risks include:
- Protein malnutrition from reduced absorption of dietary protein
- Fat-soluble vitamin deficiencies (vitamins A, D, E, and K), which can cause serious long-term consequences if unmanaged
- Persistent diarrhea and loose stools, particularly in the early months
- Higher anastomotic leak risk compared to gastric bypass, requiring close post-operative monitoring
- Lifelong, intensive supplementation — it’s non-negotiable for long-term health
Gastric bypass risks
Gastric bypass carries a more moderate risk profile, but it’s not without significant considerations:
- Dumping syndrome, which occurs in 20–50% of gastric surgery patients and causes nausea, sweating, and diarrhea after eating high-sugar or high-fat foods
- Internal hernia, a potentially serious complication that can occur years after surgery
- Nutritional deficiencies in iron, B12, and calcium, requiring lifelong supplementation
- Pouch dilation over time, which can lead to gradual weight regain
- Weight regain risk, particularly without sustained lifestyle support
Long-term nutritional considerations for both
Neither procedure is compatible with a set-it-and-forget-it approach. A systematic review of over 3,400 duodenal switch patients found that more than half developed vitamin D deficiency at long-term follow-up, with similarly high rates of vitamin A, calcium, and parathyroid hormone abnormalities.
Both procedures require lifelong supplementation, regular blood work (at minimum every 3–6 months initially, then annually long-term), and close monitoring by a multidisciplinary care team. At Everself, post-procedure patients are supported through a 12-month concierge care program designed around exactly this kind of ongoing follow-up.
Recovery: What to Expect After Each Surgery
Duodenal switch recovery
- Hospital stay: 3–5 days
- Liquid diet phase: 2–4 weeks post-discharge
- Return to normal activity: 4–6 weeks
- Follow-up monitoring: Blood work every 3–6 months in year one, then adjusted based on labs
The dual nature of this procedure makes the recovery period more demanding. Digestive adjustment takes time, and some patients experience significant changes to bowel habits in the first several months.
Gastric bypass recovery
- Hospital stay: 2–3 days
- Liquid diet phase: 2–3 weeks post-discharge
- Return to work: Typically 2–3 weeks for desk-based roles
- Follow-up monitoring: Quarterly nutritional monitoring in year one
Most patients tolerate gastric bypass recovery well. The key discipline in the early weeks is following the staged diet progression moving from liquids to soft foods to regular solids on the schedule your surgeon and dietitian provide.
Questions to Ask Your Surgeon
Before committing to either procedure, it helps to walk into your consultation with clear questions. These aren’t a substitute for medical advice, but they’re a strong starting point:
- Am I a better candidate for the duodenal switch or gastric bypass based on my BMI and health history?
- How will this procedure affect my existing comorbidities, particularly diabetes, hypertension, or GERD?
- What does my lifelong supplementation plan look like, and how often will I need blood work?
- What is your personal volume with this procedure, and what are your outcomes?
- Are there non-surgical alternatives I should consider given my BMI and goals?
- What does the revision pathway look like if I experience weight regain?
At Everself, our team can help you map your full range of options — surgical and non-surgical — so you walk into any consultation already informed.
What to Do Next
If you’re comparing the gastric bypass surgery vs duodenal switch, you’re already doing the most important thing: learning how each option works before making a decision.
Both procedures can lead to meaningful weight loss, but they come with different trade-offs. The duodenal switch tends to produce greater weight loss, while gastric bypass offers a more moderate balance between results and long-term nutritional management. Both are permanent procedures that require lifelong lifestyle and medical follow-up.
So before moving forward, it helps to think through a few key questions:
- What level of weight loss are you hoping to achieve?
- How comfortable are you with long-term nutritional monitoring and supplementation?
- Do you want to explore options that don’t involve traditional bariatric surgery?
For some patients, especially those with a BMI between 30 and 45, ESG Stomach Tightening® at Everself offers a one-time, non-surgical option that supports meaningful weight loss without incisions or intestinal rerouting.
Surgery is the right path for some. A non-surgical approach is the right path for others. What matters most is walking into your decision with the full picture.
Schedule a consultation with the Everself team to compare your options.

