Gastric Bypass vs. Lap Band: Key Differences & Results
Comparing gastric bypass vs. lap band? See how they differ in weight loss, risks, reversibility, and long-term outcomes - plus a non-surgical option.


Global leader in endoscopic weight loss, Triple-board-certified in obesity
When you start researching weight loss surgery, the gastric bypass vs. lap band comparison comes up fast. On the surface, the choice can seem simple: one procedure is highly effective but permanent, while the other appears adjustable and less invasive.
Over time, however, long-term outcomes have revealed important differences between them.
This guide explains how each procedure works, what results patients typically see, and the tradeoffs to consider when choosing the approach that best fits your health and goals.
How Each Procedure Works
Gastric bypass (RYGB)
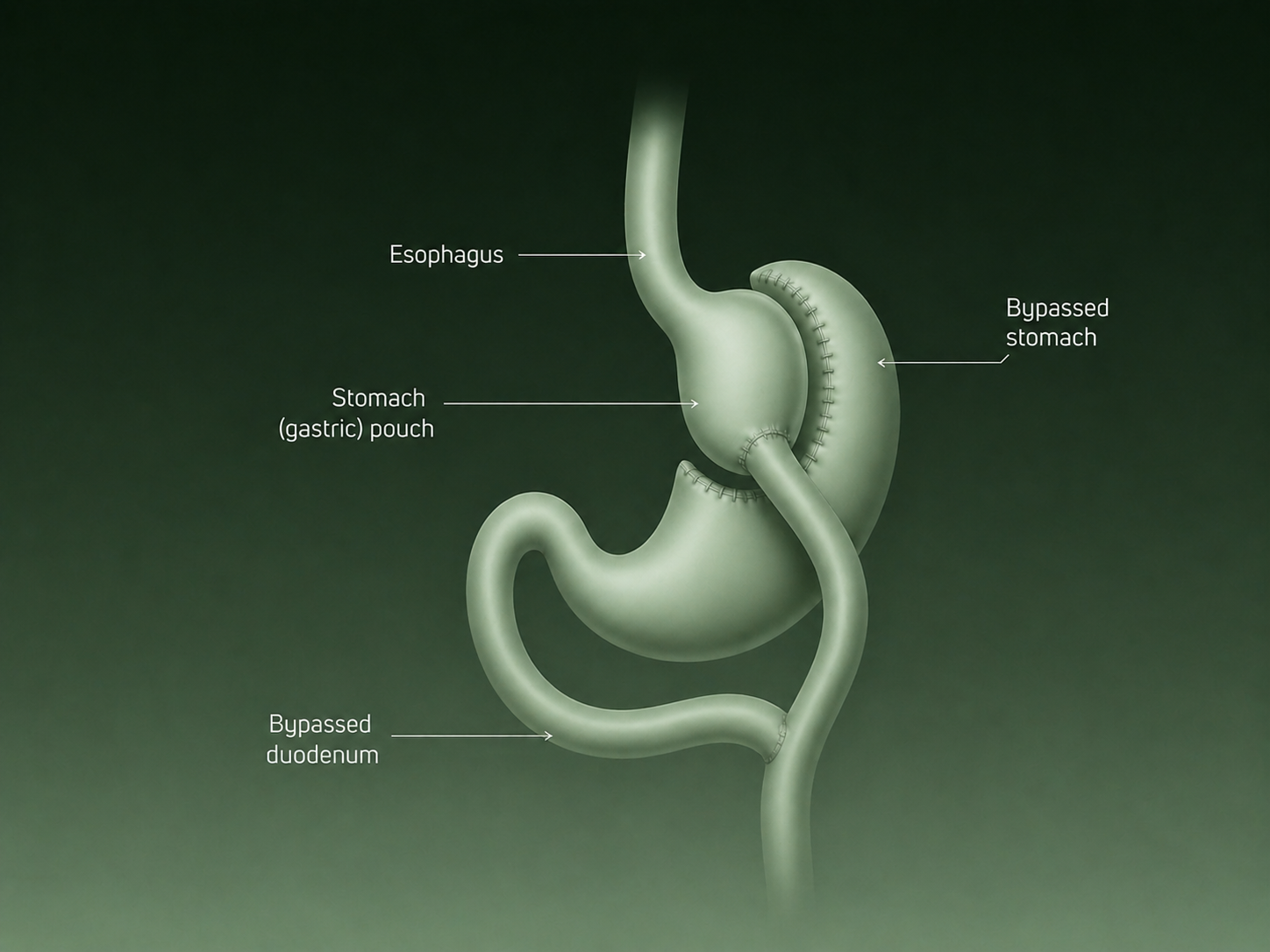
The surgeon creates a small stomach pouch and reroutes the small intestine to connect directly to it — bypassing most of the original stomach and upper small intestine.
Roux-en-Y gastric bypass (RYGB) is a two-part procedure. First, the surgeon creates a small stomach pouch, roughly the size of an egg. Then they reroute the small intestine to connect directly to this new pouch, bypassing most of the original stomach and the upper small intestine.
This dual mechanism of restriction and malabsorption is what makes gastric bypass so effective. Food intake drops significantly, and the body absorbs fewer calories. Hormonal changes also occur rapidly, which is why many patients see improvements in blood sugar and blood pressure within days of surgery, often before significant weight loss has taken place.
| 💡 Quick note: Patients often confuse gastric bypass with gastric sleeve surgery. While both are bariatric procedures, they work differently. Gastric sleeve removes a large portion of the stomach, whereas gastric bypass changes both stomach size and the path food takes through the digestive system. If you’re comparing the two, our guide on gastric sleeve vs gastric bypass explains the differences in more detail. |
|---|
Lap band (LAGB)
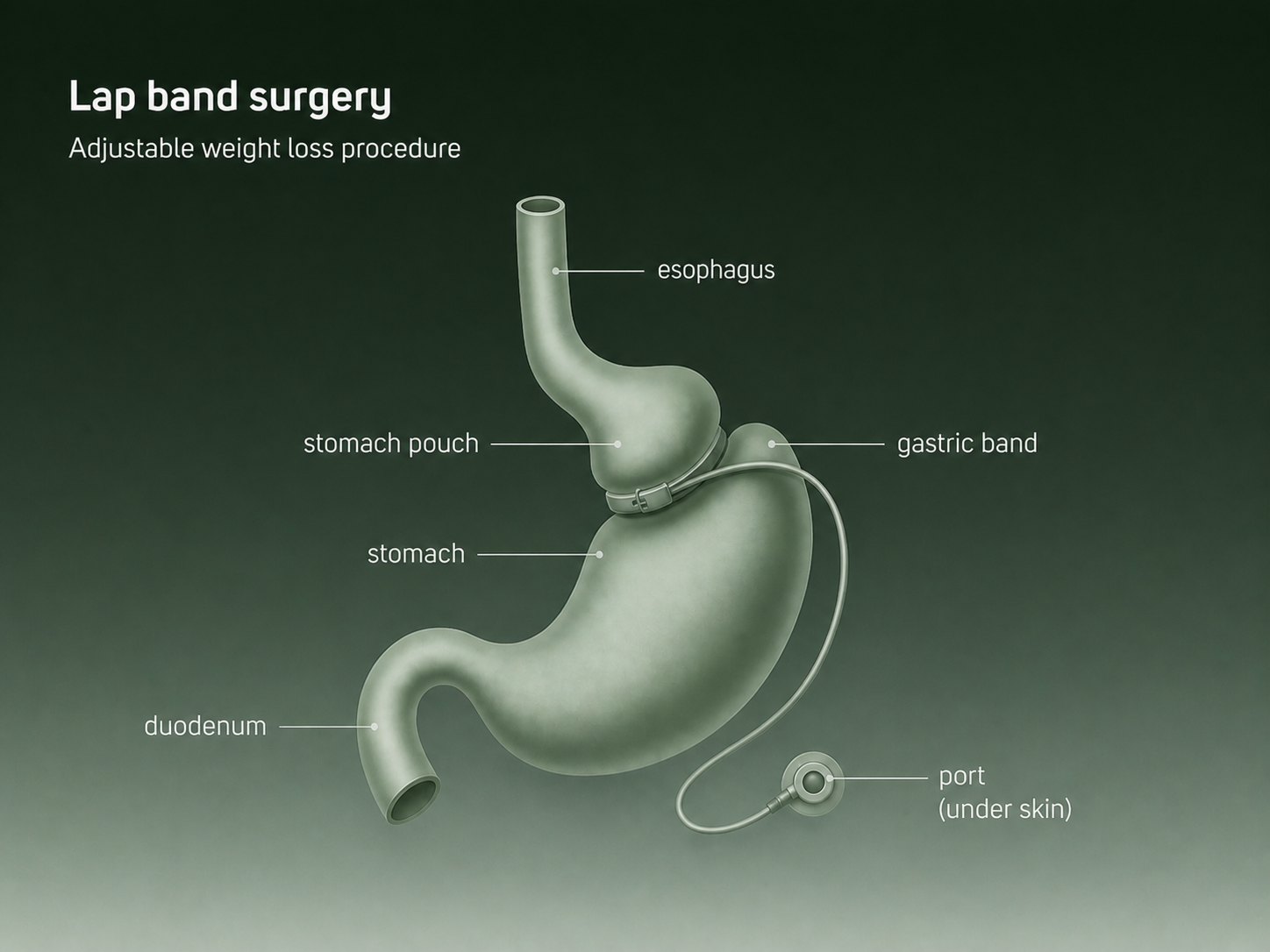
An adjustable silicone band is placed around the upper stomach to create a small pouch — slowing food intake and promoting fullness, with no rerouting or tissue removal.
The laparoscopic adjustable gastric band (LAGB) works differently. A silicone band is placed around the upper portion of the stomach, creating a small pouch above it. The band is connected to a port just under the skin and can be tightened or loosened via saline injections.
The mechanism is purely restrictive: the band slows how quickly food passes through, helping patients feel full sooner. There’s no intestinal rerouting, no removal of stomach tissue, and no hormonal component. That simpler profile once made lap band appealing. Over time, it’s also what limits it.
For patients evaluating lap band vs gastric bypass, this difference in mechanism, that is, restriction alone versus restriction plus metabolic changes, plays a major role in long-term outcomes.
Who Is a Good Candidate for Each Procedure?
When patients research gastric bypass vs lap band, candidacy often becomes one of the first questions they ask. Understanding who tends to benefit most from these procedures helps patients and clinicians determine whether this procedure is an appropriate option.
Gastric bypass candidates
Current bariatric surgery guidelines emphasize that candidacy should be based on both body weight and the presence of obesity-related health conditions.
In general, gastric bypass is recommended for adults with severe obesity, typically those with a BMI of 40 or higher. It is also commonly considered for patients with a BMI of 35 or higher who are living with obesity-related conditions such as type 2 diabetes, hypertension, sleep apnea, or other metabolic diseases. These individuals often benefit from the metabolic effects of surgery, which can improve or even help resolve certain conditions alongside weight loss.
The updated guidelines also acknowledge that metabolic disease severity matters. In some cases, patients with a BMI below traditional thresholds may still be considered for metabolic surgery if they have poorly controlled type 2 diabetes or other serious obesity-related conditions.
Lap band candidates
When lap bands were more widely recommended, the typical candidate was someone with a BMI between 35 and 45 who wanted a reversible, less invasive option. The procedure’s adjustability was seen as an advantage, allowing clinicians to fine-tune restriction over time.
In practice, that promise hasn’t held up well. Many patients require frequent office visits for adjustments, and a significant number eventually face band slippage, erosion, esophageal dilation, or outright failure. For this reason, many bariatric surgeons have moved away from recommending it as a first-line option.
When surgery may not be the right first step
Not every patient needs or wants traditional bariatric surgery, and for many, it isn’t the only credible option.
If your BMI is on the lower end of the bariatric range, you’re concerned about permanent anatomical changes, or you want to be back on your feet within days rather than weeks, a non-surgical path may be worth exploring.
ESG Stomach Tightening® is a one-time, non-surgical minimally invasive and reversible endoscopic procedure approved for patients with a BMI of 30 or higher, a lower threshold than either gastric bypass or lap band. It uses sutures placed through a flexible endoscope to reshape the stomach from the inside, reducing its capacity without incisions, implanted devices, or intestinal rerouting.
For patients with a BMI between 30 and 45 who want durable results and a faster recovery, ESG is the least invasive weight loss surgery.
Weight Loss Results: What the Data Actually Shows
Weight loss surgery results tend to follow a predictable pattern: the largest drop usually happens in the first one to two years, followed by a slower maintenance phase. If you’re exploring weight loss surgery options, it helps to compare how each procedure affects anatomy, recovery time, and long-term durability.
For many patients researching lap band surgery vs gastric bypass, long-term device durability becomes a key factor in their decision.
A long-running prospective study of bariatric surgery patients found clear differences between the two procedures over time.
Year 1–2: Peak weight loss
The first year is when most patients see the fastest progress. Typical outcomes:
Gastric bypass
- 28–32% total body weight loss at peak, typically reached between 12–24 months
- Weight loss usually peaks between 12–24 months
Lap band
- ~15–20% total body weight loss
- Results depend heavily on band adjustments and follow-up care
Around 5 years: Results begin to diverge
At mid-term follow-up, the difference between procedures becomes more noticeable.
Gastric bypass
- Most patients maintain a large portion of their early weight loss
- Long-term maintenance tends to remain strong
Lap band
- Results become more variable
- Some patients maintain weight loss, while others experience regain or require device adjustments
10 years and beyond: Durability matters
Long-term data highlights the biggest difference between the procedures. In long-term follow-up from the Swedish Obese Subjects study:
| Procedure | Average long-term weight loss |
|---|---|
| Gastric bypass | ~25% weight loss from baseline |
| Gastric banding | ~14% weight loss from baseline |
These results show that gastric bypass tends to maintain nearly double the long-term weight loss of banding procedures.
Gastric Bypass vs. Lap Band: Side-by-Side Comparison
This is where the gastric bypass vs lap band comparison becomes clearer, when you look at long-term data side by side.
| Gastric Bypass (RYGB) | Lap Band (LAGB) | ESG Stomach Tightening® | |
|---|---|---|---|
| How it works | Stomach pouch + intestinal rerouting | Silicone band around stomach | Endoscopic sutures reshape stomach |
| %TWL at 1 year | 28–32% | 15–20% | 15–20% |
| %TWL at 5 years | 25–30% | Highly variable | 15–20% |
| Reversibility | No | Yes (device removal) | Revisable (sutures can be adjusted) |
| Implanted device | No | Yes | No |
| Recovery time | 2–4 weeks | 2–4 weeks | 2–3 days |
| Incisions | Yes (laparoscopic) | Yes (laparoscopic) | None |
| Intestinal rerouting | Yes | No | No |
| Minimum BMI | 35–40 | 35–40 | 30 |
| Long-term durability | Strong | Weakens over time | Moderate, well supported |
| Ongoing maintenance | Low | High (frequent adjustments) | Low with lifestyle |
Risks and Complications
Gastric bypass risks
Gastric bypass is major surgery and carries real risks. These include anastomotic leaks, dumping syndrome, nutritional deficiencies (particularly iron, B12, calcium, and vitamin D), and marginal ulcers. Because the intestinal anatomy is permanently altered, lifelong supplementation is typically required.
Dumping syndrome, in which food moves too quickly into the small intestine, affects an estimated 25–50% of gastric bypass patients to some degree. For most, dietary adjustments manage symptoms effectively.
Lap band risks
Lap band complications divide into early and late categories. Early risks include port site infection, band slippage, and difficulty swallowing. Late complications are where the procedure’s track record becomes more concerning: esophageal dilation, band erosion into the stomach wall, and port malfunction are all documented in long-term follow-up data.
The frequent saline adjustments required to maintain appropriate restriction also mean ongoing access to a skilled bariatric center. For patients in areas with limited follow-up resources, outcomes tend to be worse.
The lap band’s long-term track record
Long-term data on adjustable gastric banding shows mixed durability. In a 15-year randomized study, complications occurred in about 18.4% of patients, including band erosion, slippage, and port-related issues, with some patients requiring band removal or conversion to another procedure.
The study also found that improvements in obesity-related conditions seen at five years often declined by the 15-year follow-up, suggesting more limited long-term durability for gastric banding.
Some patients still do well with lap bands, particularly with consistent follow-up and adjustments. But population-level data suggests outcomes can be less predictable over the long term compared with procedures like gastric bypass.
Reversibility and Adjustability: Does It Matter?
Reversibility is one of the main reasons patients have historically chosen lap band over other options. The idea of a “removable” procedure appeals to people who are uncertain about permanent changes, and that’s understandable.
The nuance worth knowing is this: “removable” does not mean “consequence-free”.
A lap band can be taken out, but the underlying weight doesn’t disappear with it. Patients who have their bands removed without transitioning to another intervention often regain the weight they lost. In that sense, the band’s reversibility can become a liability if complications force removal prematurely.
For patients drawn to reversibility because they want to avoid a permanent device or permanent anatomical changes, ESG Stomach Tightening® addresses both concerns at once. It’s a one-time, non-surgical endoscopic procedure with no implanted hardware or removed stomach tissue. The sutures can be revised if needed, and the stomach’s natural anatomy remains intact.
What If You Already Have a Lap Band?
If you have a lap band and it’s not working the way it once did, you’re not alone. Band failure is one of the most common reasons patients seek bariatric revision, and it’s not a reflection of personal failure. Devices wear out, slip, erode, or simply stop providing adequate restriction as anatomy changes over time.
The first step is an honest evaluation. A bariatric specialist can assess whether your band is still correctly positioned, whether it’s causing silent damage (esophageal dilation in particular can worsen without obvious symptoms), and whether removal, conversion, or a less invasive alternative makes more sense given your current health status.
Common revision paths include:
- Conversion to gastric bypass: The most studied revision after lap band. Generally produces stronger weight loss than converting to a sleeve.
- Conversion to gastric sleeve: Less commonly recommended after band removal, given GERD risk.
- ESG Stomach Tightening®: For patients who want a non-surgical path after band removal, ESG may be appropriate depending on BMI, stomach anatomy, and health history. A consultation can determine candidacy.
Choosing the best alternative for you
Choosing between gastric bypass and lap band surgery ultimately comes down to how much weight loss you’re aiming for, how durable you want the results to be, and what level of intervention feels right for you.
Gastric bypass has a long track record of producing substantial and sustained weight loss, along with meaningful improvements in obesity-related health conditions. Lap band surgery, while adjustable and less invasive at the outset, tends to produce more modest and variable long-term results and often requires ongoing management over time.
To help narrow it down:
- Gastric bypass may be the right fit if you have a BMI of 40 or higher, significant obesity-related health conditions, and are looking for the most durable long-term results available.
- Lap band is rarely a first recommendation today but may still be considered if you have specific medical reasons that rule out more effective options. If you already have one and it’s not working, revision is worth discussing.
- ESG Stomach Tightening® is worth exploring if you want meaningful, lasting weight loss without surgery, a permanent implant, or a lengthy recovery particularly if your BMI falls between 30 and 45.
For patients who want a less invasive approach without a permanent device, the better comparison today may be between gastric bypass and ESG Stomach Tightening®, not between gastric bypass and lap band.
If you’re in the BMI 30–45 range and want to explore a non-surgical path, we’d love to talk.

