Mini Gastric Bypass vs Gastric Bypass: Key Differences Explained
Weighing mini gastric bypass vs gastric bypass? Compare risks, recovery, and understand why many patients choose a non-surgical path instead.

Global leader in endoscopic weight loss, Triple-board-certified in obesity
You didn’t end up on this page by accident. You’ve probably spent hours reading, researching, maybe lying awake, wondering whether a major surgery is really the only path forward.That discomfort you feel, not just in your body but in the decision itself, is something many patients carry quietly. The fear of going under general anesthesia. The worry about permanent changes you can’t undo. The hope that there’s a way to feel like yourself again without giving up weeks of your life to recovery.
This article is for you. It covers two commonly compared procedures: mini gastric bypass and Roux-en-Y gastric bypass, honestly and without the clinical hedge. It also introduces a non-surgical alternative that’s worth understanding before you decide on anything.
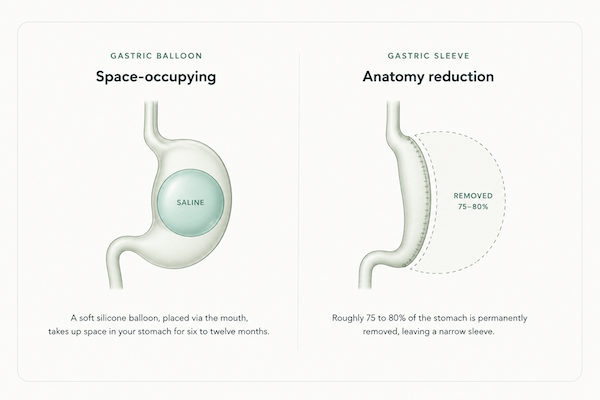
What Is A Gastric Bypass (Roux-en-Y)?
Roux-en-Y gastric bypass (RYGB) is one of the most studied weight-loss procedures worldwide and is widely considered the gold standard for complex bariatric cases.
During the procedure, a surgeon creates a small stomach pouch roughly the size of an egg and connects it directly to the middle section of the small intestine. This bypasses the remaining stomach and most of the upper intestine, limiting how much you can eat and how many calories your body absorbs. Hormonal changes that support weight loss follow quickly.
The operation typically takes two to three hours under general anesthesia and requires a two- to three-day hospital stay. Return to normal activity takes three to six weeks. RYGB involves two intestinal connections, known as anastomoses, which makes it surgically more complex than the mini bypass. It’s most often recommended for patients with severe GERD, type 2 diabetes, or a BMI above 40.
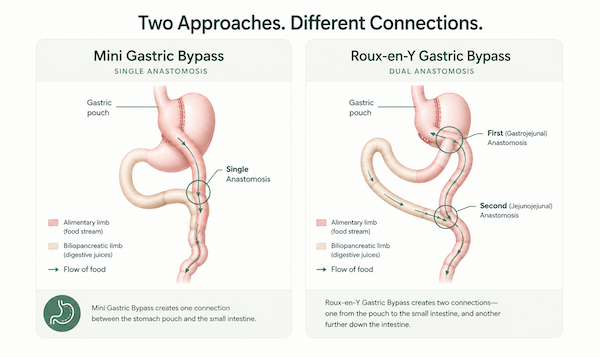
What Is a Mini Gastric Bypass?
The mini gastric bypass, also called one anastomosis gastric bypass, follows the same principle as RYGB but uses a simpler technique.
Instead of two intestinal connections, it creates just one. A long, narrow stomach pouch is formed and looped directly to the small intestine. Operative time is shorter, and surgical complexity is lower.
The name “mini” refers to surgical simplicity, not scale. Both procedures still require general anesthesia, a hospital stay, and permanent anatomical changes. For patients weighing their options, the difference between surgical and non-surgical paths is worth understanding clearly.
As Dr. Pichamol Jirapinyo, co-founder of Everself and Assistant Professor of Medicine at Harvard Medical School, notes, patients in real life often see more modest results from any intervention “due to interruptions and insurance limits,” which is why matching the right treatment to each patient’s actual circumstances matters more than the name on the procedure. For many patients with a BMI of 30–40, that means a non-surgical path deserves serious consideration before committing to irreversible surgery.
Both procedures restrict how much you can eat and reduce calorie absorption. The anatomical difference lies in how the stomach connects to the intestine and how much of the intestinal tract is bypassed. That difference has meaningful implications for risk, particularly around bile reflux.
Mini Gastric Bypass vs Gastric Bypass: Side-by-Side Comparison
For patients also considering non-surgical paths, it’s worth including ESG Stomach Tightening® in any comparison. Those exploring related procedures may also find context in our overview of gastric sleeve vs gastric bypass.
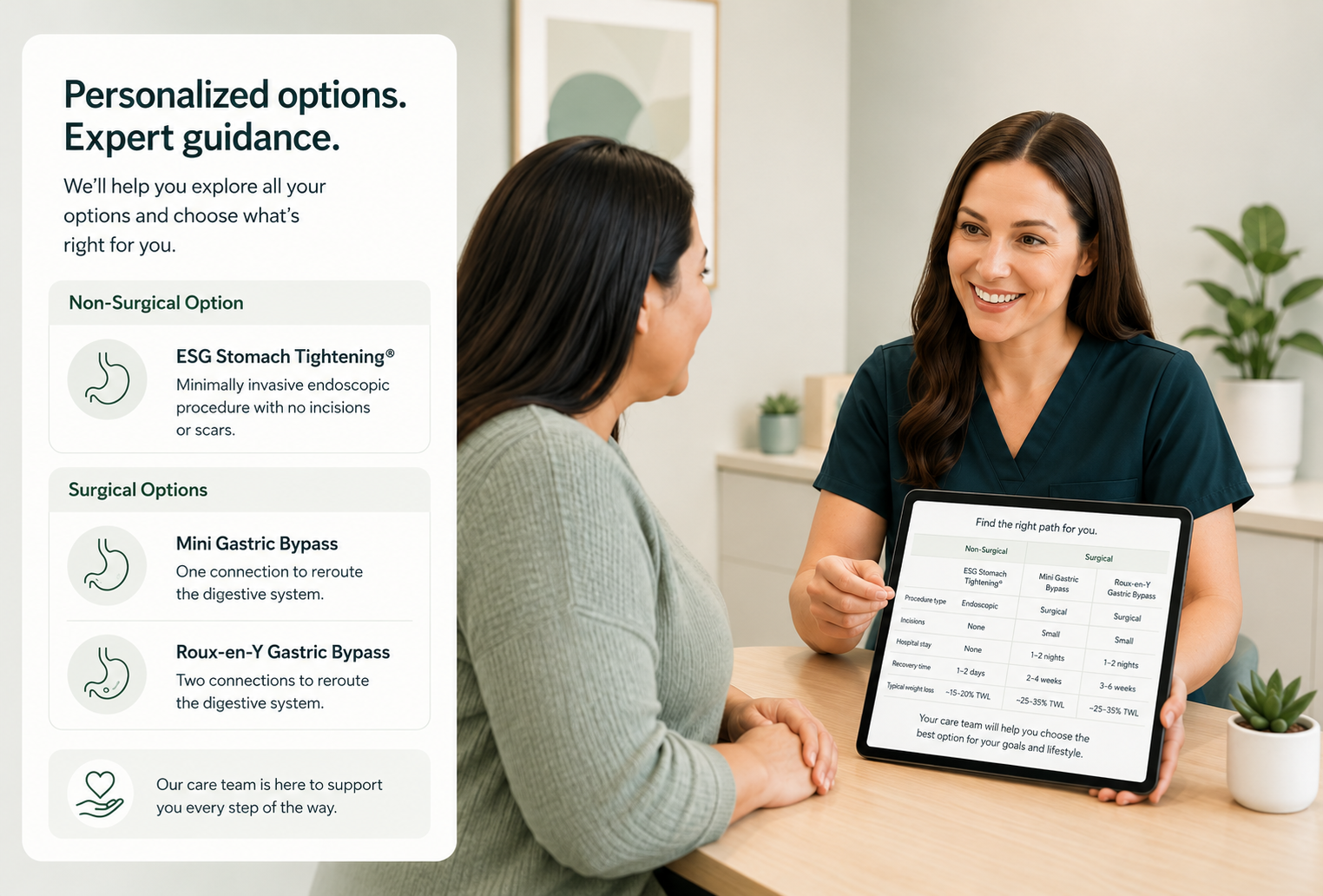
Comparison table of mini gastric bypass, Roux-en-Y gastric bypass, and ESG Stomach Tightening across key surgical and recovery metrics.
Weight Loss Results: How Do They Compare?
Both procedures produce significant weight loss, and the meaningful differences show up in the timing and the long-term curve rather than the headline number.
Short-term results (1–2 years)
Both procedures produce substantial weight loss, and their outcomes at one year are comparable. A systematic review of randomized controlled trials found that mini-bypass resulted in statistically greater total weight loss at 6 months, with no significant difference at 12, 24, or 36 months compared with RYGB.
On average, patients undergoing either procedure can expect roughly 25–35% total weight loss by the end of year one, depending on starting BMI and adherence to follow-up care.
For context, ESG Stomach Tightening® produces an average of 15–20% total weight loss at one year per published series. For many patients with a BMI between 30 and 40, that difference carries real weight alongside the significant gaps in recovery, invasiveness, and risk.
Long-term durability and regain risk
Both RYGB and mini bypass show durable results, but weight regain over five or more years is a genuine concern. Dietary habits, behavioral support, and consistent follow-up care tend to predict long-term maintenance more reliably than the surgical technique itself.
Patients who experience weight regain after bypass have options. Understanding weight regain after bariatric surgery and gastric bypass revision is a useful context for anyone weighing the long-term picture.
Risks and Complications to Know
Every surgery carries risk. Here’s what’s specific to each procedure — and what they share.
Mini gastric bypass risks
The most significant concern with mini-bypass is bile reflux. Because of the single anastomosis structure, bile can travel back into the stomach pouch and, in some cases, the esophagus. This can cause gastritis, chronic heartburn, or esophageal irritation.
For most patients, bile reflux is manageable through dietary adjustments and medication. In persistent or severe cases, a revision to a Roux-en-Y configuration may be considered. Patients with pre-existing GERD are generally not ideal candidates. Internal hernia risk, by contrast, is lower with mini bypass than with RYGB.
Roux-en-Y gastric bypass risks
RYGB carries a higher risk of internal hernia. Internal hernias occur when a loop of intestine slips through a gap created during surgery, which can cause serious complications requiring emergency intervention.
Additional risks include anastomotic strictures (narrowing at the connection sites), dumping syndrome, and nutritional deficiencies requiring lifelong supplementation. The surgical complexity of RYGB, with two intestinal connections, carries a slightly higher complication profile, particularly involving leaks or strictures.
Risks they share
For all the differences between these two procedures, what they share matters just as much:
- Both are irreversible or extremely difficult and risky to reverse
- Both require general anesthesia and a hospital stay
- Both involve permanent anatomical changes to the digestive tract
- Both carry the risk of nutritional deficiencies requiring lifelong monitoring
- Both require a recovery measured in weeks, not days
These shared risks are worth weighing carefully, particularly for patients considering whether the least invasive weight-loss procedure might be a better fit.
Illustration of common post-bariatric surgery considerations, including bile reflux, internal hernia risk, and the need for lifelong nutritional supplementation.
Recovery: What to Expect After Each Procedure
Recovery timelines for both procedures are nearly identical:
- Hospital stay: Two to three days
- Return to light activity: One to two weeks
- Return to normal activity: Three to six weeks
- Full dietary progression (liquid to soft to solid): Six to eight weeks
For people managing work, family, or caregiving responsibilities, the three to six weeks of restricted activity is a real commitment, not a formality. Pain management, wound care, and strict dietary phases are part of the process for both.
Want to compare that to a two- to three-day recovery with no incisions? Explore ESG Stomach Tightening®.
Is There a Non-Surgical Alternative to Both?
For patients with a BMI in the 30–40 range who want meaningful weight loss without surgery, ESG Stomach Tightening® is worth understanding in detail.
What is ESG Stomach Tightening®?
ESG Stomach Tightening® is a one-time, non-surgical endoscopic procedure that reduces stomach volume by up to 70–80% from the inside using a flexible endoscope and an internal suturing device. Unlike the gastric sleeve, ESG involves no external incisions, no scars, and no permanent changes to the digestive tract’s anatomy.
It’s performed as an outpatient procedure, with no incisions and no hospital admission. Most patients go home the same day and return to normal activity within two to three days. It was pioneered by Dr. Christopher Thompson, Professor of Medicine at Harvard Medical School and Everself co-founder, who performed the first ESG Stomach Tightening® cases worldwide in 2012 and has since completed more than 6,000 endoscopic weight-loss procedures.
How ESG weight loss compares
Peer-reviewed longitudinal data show ESG patients achieving an average of approximately 16% total weight loss at 5 years, with 10-year follow-up data indicating durable results of 15.8% TWL. There is no intestinal rerouting, no bile reflux risk, no internal hernia risk, and no permanent anatomical changes.
ESG produces less total weight loss than mini bypass or RYGB on average. For patients with a BMI above 40, severe GERD, or obesity-related conditions where maximum weight loss is medically necessary, bariatric surgery may remain the stronger clinical recommendation. ESG is built for a different patient profile, the BMI 30–40 range where the tradeoffs between outcomes and invasiveness can shift the math meaningfully in favor of a non-surgical path.
Patients considering all their options may also find it helpful to review the safest weight-loss surgery options before deciding.
Who is ESG right for?
ESG is generally appropriate for adults with a BMI between 30 and 40 who:
- Prefer to avoid general anesthesia, incisions, or permanent anatomical changes
- Need minimal downtime due to work or caregiving responsibilities
- Want meaningful, durable weight loss from a one-time procedure
- Are concerned about surgical complications or long-term bypass-related risks
The Everself Program pairs every ESG procedure with 12 months of concierge support from a multidisciplinary care team: registered dietitians, nurse practitioners, and coaches who stay engaged through the year your habits and metabolism are most actively recalibrating. The single biggest predictor of long-term success after any weight loss procedure is consistent follow-up, and that’s exactly what most surgical programs leave you to figure out alone after the first six weeks.
“I’m almost a year out since my ESG procedure, and it’s been a complete life-changer. 100% recommended. I started out weighing 197 lbs. and prediabetic; a year later, I weigh 133 lbs.” — Maria N., ESG Stomach Tightening® patient. Source: everself.com
See whether ESG Stomach Tightening® is right for you — book your consultation.
Which Procedure Is Right for You?
The right answer depends on your health profile, your goals, and what tradeoffs you’re willing to accept — not on which article you happened to read last.
Roux-en-Y gastric bypass may be the stronger clinical choice for patients with severe GERD, type 2 diabetes, or a BMI above 40 who have been evaluated by a bariatric specialist and need maximum weight loss outcomes.
Mini gastric bypass may suit patients seeking a shorter operative time and lower risk of internal hernia, while accepting the higher bile reflux risk associated with a single anastomosis.
ESG Stomach Tightening® is worth a serious look for patients with a BMI of 30–40 who want meaningful, durable weight loss without surgery, hospital admission, or the weeks of recovery both bypass procedures require. For this patient profile, the American Society for Metabolic and Bariatric Surgery includes ESG in its guidance on endoscopic weight loss procedures.
None of these decisions should be made from an article alone. A personalized consultation gives you the full picture — your candidacy, your risks, and the path that genuinely aligns with your health and life.
Not sure which path is right for you? Let’s talk. Our team can walk you through your options in a personalized consultation.
An Everself care team member reviewing non-surgical and surgical weight loss options with a patient to support a confident, informed treatment decision.
Frequently Asked Questions
Is mini gastric bypass safer than gastric bypass?
Neither is risk-free. Mini bypass carries a lower internal hernia risk than RYGB but a higher risk of bile reflux, which can cause chronic stomach irritation or esophageal inflammation. Overall, surgical complexity is slightly lower for mini bypass due to its single-anastomosis technique, but both procedures involve general anesthesia, permanent anatomical changes, and a comparable complication profile. The right choice depends heavily on your specific medical history — particularly your GERD status and BMI.
Which has better weight loss results: mini bypass or traditional gastric bypass?
Both produce comparable weight loss, averaging roughly 25–35% of total body weight at one year. A systematic review found that mini-bypass resulted in greater total weight loss at 6 months, with no statistically significant difference at 12, 24, or 36 months. Long-term durability depends more on follow-up care, dietary habits, and behavioral support than on the specific technique.
Can a mini gastric bypass be reversed?
Technically, it can be converted to another configuration, but it’s not routine. Like RYGB, mini bypass involves permanent anatomical changes that are difficult and risky to undo. It should be approached as a lifelong decision.
What is the recovery time for a mini gastric bypass?
Most patients spend two to three days in the hospital. Return to light activity typically takes one to two weeks; full recovery to normal activity takes three to six weeks, with dietary progression from liquids to soft foods to solids over six to eight weeks.
What is the non-surgical alternative to gastric bypass?
ESG Stomach Tightening® is the most established non-surgical endoscopic alternative for patients who want meaningful weight loss without surgery. It’s a one-time procedure with no incisions, no general anesthesia, and a two- to three-day recovery.Published data show durable results out to 10 years. It’s most appropriate for patients with a BMI of 30–40. Schedule a consultation to explore whether it’s the right fit for you.