Which Bariatric Surgery is Best for PCOS: ESG vs Sleeve vs Bypass
Compare gastric sleeve, bypass, and non-surgical ESG for weight loss, fertility, insulin resistance. Find the best fit for PCOS symptoms.


Global leader in endoscopic weight loss, Triple-board-certified in obesity
If you have PCOS and you’ve been told to “just lose weight,” you already know how much easier that is to say than to do. Polycystic ovary syndrome (PCOS) drives insulin resistance, hormonal imbalance, and weight gain that resists standard dieting. For many women, medical weight loss support is the only path that actually works.
Studies published in journals like Obesity Surgery and The Journal of Clinical Endocrinology & Metabolism show that even moderate weight loss can restore menstrual cycles, lower androgen levels, improve insulin sensitivity, and significantly increase fertility outcomes in women with PCOS. But not all weight loss methods deliver these results equally and for PCOS patients, those differences matter.
This guide answers which bariatric surgery is best for PCOS by comparing the most common procedures side by side like gastric sleeve, gastric bypass, ESG Stomach Tightening®, and gastric balloon. By the end, you’ll have a clear picture of which approach fits your goals.
Why Bariatric Procedures Can Help PCOS Symptoms
PCOS is fundamentally a metabolic condition. Excess weight amplifies insulin resistance, which drives up androgen levels and disrupts ovulation. It’s a cycle and weight loss can break it.
For many women exploring pcos and weight loss surgery, bariatric and endoscopic procedures stand out because they create sustained, clinically meaningful weight loss—something that’s difficult to achieve and maintain with diet or medication alone. Beyond weight loss, these procedures also trigger early metabolic shifts.
Improvements in insulin sensitivity and inflammation often begin within weeks, well before visible weight changes, setting the stage for faster hormonal recovery.
Gastric Sleeve for PCOS: Pros, Cons, and Outcomes
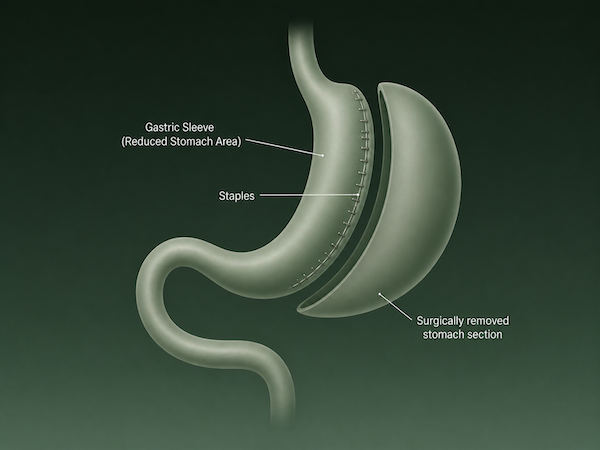
PCOS Gastric sleeve surgery reduces stomach size by removing a large portion, creating a narrow tube that limits food intake.
When evaluating which bariatric surgery is best for PCOS, gastric sleeve is often one of the first options considered due to its strong and consistent outcomes. Gastric sleeve surgery (sleeve gastrectomy) removes roughly 75–80% of the stomach, leaving a narrow tube. It’s one of the most commonly performed bariatric procedures globally and has a strong evidence base for improving PCOS-related symptoms.
For PCOS patients, typical outcomes include 20–30% total body weight loss within the first year, along with improvements in menstrual regularity, insulin resistance, and androgen levels. The degree of weight loss, rather than starting BMI, is what most strongly influences whether cycles normalize after surgery. In other words, the results depend less on where you start and more on how much metabolic change the procedure helps you achieve.
In a large cohort study, nearly 79% of women experienced remission of irregular menstrual cycles within a year, alongside an average weight loss of around 33% of total body weight.
What makes it a strong option
- Produces significant, durable weight loss
- Ghrelin reduction improves long-term appetite control
- Well-studied for metabolic and hormonal outcomes in PCOS
What to weigh carefully
- Permanent and irreversible — part of the stomach is removed
- Surgical risks: general anesthesia, staple-line leaks, infection, scarring
- Recovery takes 3–6 weeks; hospital stay required
- Can worsen or trigger GERD (acid reflux) in some patients
- Does not correct malabsorption, but also doesn’t cause it
For women with PCOS who are planning a pregnancy, the permanence of sleeve surgery is worth weighing carefully. Nutritional adequacy during conception and pregnancy is a real consideration post-sleeve.
Gastric Bypass for PCOS: Stronger Hormone Reset?
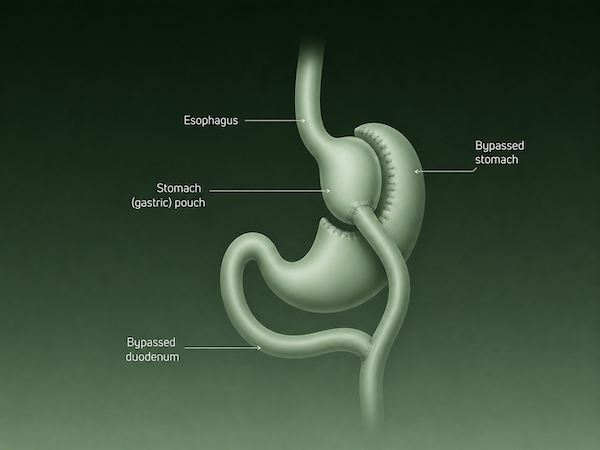
Gastric bypass creates a small stomach pouch and reroutes the small intestine, altering digestion and nutrient absorption.
Gastric bypass (Roux-en-Y) works differently from other procedures. It reduces stomach size by rerouting part of the small intestine changing how the body absorbs nutrients and regulates hormones. This dual mechanism makes it one of the most metabolically active bariatric procedures.
Clinical evidence shows that gastric bypass leads to stronger early improvements in blood sugar control compared to sleeve surgery, with higher rates of diabetes remission in the first year. This is driven by rapid hormonal changes in the gut that improve insulin sensitivity almost immediately after surgery.
For women with PCOS where insulin resistance is a key driver, this matters. A more aggressive metabolic shift can translate into faster improvements in ovulation, androgen levels, and cycle regularity, especially in those with severe insulin dysfunction or PCOS-related diabetes.
When bypass may be the right fit
- Severe insulin resistance or PCOS-related type 2 diabetes
- BMI 40+ or BMI 35+ with significant metabolic comorbidities
- Prior procedures that haven’t produced sufficient results
What to weigh carefully
- Malabsorption is lifelong; supplementation (iron, B12, calcium, vitamin D) is required
- Nutritional deficiencies during pregnancy are a real concern—planning is essential
- Higher surgical complexity and longer recovery than sleeve
- Irreversible without major revision surgery
Gastric bypass offers one of the most powerful metabolic resets available, but it comes with equally significant long-term nutritional demands. For women with PCOS planning pregnancy, timing, monitoring, and medical guidance become critical.
Other Surgical Options: Band and Duodenal Switch
Gastric band (lap-band): Once common, now largely phased out. Weight loss is modest (15–25% %TWL), band-related complications are frequent, and PCOS outcomes are limited compared to newer options. Most specialists no longer recommend it as a first-line choice.
Duodenal switch (BPD/DS): The most aggressive bariatric procedure and the most powerful for metabolic disease. Produces up to 35–45% %TWL but carries the highest nutritional risk. Rarely recommended unless other options have failed and metabolic severity is extreme. Not typically appropriate for women planning pregnancy in the near term.
ESG Stomach Tightening® for PCOS: The Non-Surgical Alternative
.BOBSzfOb_Z1S5OvN.png)
ESG reduces stomach volume using internal sutures placed via endoscope, without incisions or tissue removal.
ESG Stomach Tightening® is a one-time, non-surgical endoscopic procedure that reduces stomach size from the inside using sutures placed through a flexible endoscope. No incisions or scars. No removal of stomach tissue.
For women with PCOS, it represents a meaningful path forward, particularly those prioritizing fertility, minimal recovery, and the ability to avoid the risks of traditional surgery.
How it works
An endoscope is passed through the mouth into the stomach. A suturing device creates a series of internal stitches, reducing stomach volume by roughly 70–75%. Patients feel full sooner, eat less, and lose weight over time without any permanent anatomical change.
What the evidence shows for PCOS
- Average 15–20% %TWL, with strong results in patients who engage with follow-up support
- Meaningful improvements in insulin sensitivity, fasting glucose, and cholesterol
- Menstrual cycle restoration has been documented in ESG studies involving women with obesity-related hormonal disruption
- No malabsorption means no elevated nutritional risk during conception or pregnancy
Why ESG is particularly well-suited to PCOS patients planning a family
Fertility is a priority for many women with PCOS. Before proceeding, it’s important to weigh the ESG pros and cons for PCOS. ESG delivers weight loss that can meaningfully restore hormonal balance without the nutritional concerns of bypass or the irreversibility of sleeve. Recovery is measured in days. Most patients return to normal activity within 2–3 days.
The non-surgical benefits for PCOS symptoms are no scar tissue, no malabsorption risk, and a body that remains anatomically intact for pregnancy.
Gastric Balloon for PCOS: Temporary Boost

A gastric balloon occupies space in the stomach, helping patients feel full sooner and reduce calorie intake.
The gastric balloon is a non-surgical, reversible option designed to kickstart weight loss. A soft silicone balloon is placed inside the stomach, where it takes up space and helps you feel full sooner. Depending on the type, it typically remains in place for a few months before being removed or naturally passing.
Clinical data shows patients can lose around 14% of total body weight within 4 months, alongside measurable improvements in metabolic health markers like blood sugar and cholesterol. These early shifts are often enough to begin improving cycle regularity and insulin sensitivity.
What makes the balloon particularly useful is its role as a starting point. Because the weight loss happens rapidly, it can help break through metabolic resistance and create momentum both physiologically and behaviorally. Some patients are also able to maintain a portion of that weight loss after the balloon is gone, especially with structured follow-up.
Who it fits well
- Women who want a reversible, lower-commitment starting point
- Those not yet ready for ESG or surgery, but wanting a clinical intervention
- PCOS patients using it as a bridge to reach a healthier weight before conception
- Patients looking to build sustainable habits with medical support
The balloon doesn’t deliver the same long-term weight loss as ESG or surgical options, but as a catalyst for metabolic improvement and habit formation, it can be highly effective for the right patient especially early in the PCOS treatment journey.
Comparison Table: Best Procedure for Your PCOS Goals
If you’re still unsure which bariatric surgery is best for PCOS, comparing these options side by side makes the differences clearer.\
| Procedure | Avg %TWL | PCOS/Fertility Impact | Recovery | Reversible? | Surgical Risks | Best For |
|---|---|---|---|---|---|---|
| ESG Stomach Tightening® | 15–20% | Strong: insulin, cycles, fertility | 2–3 days | Yes (sutures can be revised) | Minimal | PCOS + fertility goals, BMI 30+ |
| Gastric Sleeve | 20–30% | Strong: insulin, testosterone | 3–6 weeks | No | Moderate | Higher BMI, not planning near-term pregnancy |
| Gastric Bypass | 25–35% | Strongest metabolic reset | 4–8 weeks | No | Higher | Severe insulin resistance/diabetes + PCOS |
| Gastric Balloon | 10–15% | Moderate: cycle improvement | 1–2 days | Yes (removed at 6 months) | Minimal | Lower BMI, reversible jump-start |
| Lap-Band | 15–25% | Limited | 1–2 weeks | Yes | Low-moderate | Largely outdated; rarely recommended |
Key Factors for PCOS Patients Choosing a Procedure
Ultimately, deciding which bariatric surgery is best for PCOS depends on how these factors align with your health, timeline, and long-term goals.
BMI and metabolic severity
ESG is approved for BMI 30+, making it accessible to far more PCOS patients than surgical options (which typically require BMI 35–40+). Women with severe insulin resistance or PCOS-related diabetes may benefit from bypass’s stronger metabolic action.
Fertility timeline
If you’re planning to conceive within 12–24 months, the reversibility and nutritional safety of ESG make it a clinically preferred option over bypass. Sleeve patients are generally advised to wait 12–18 months post-surgery before attempting pregnancy. ESG patients face fewer nutritional constraints.
Recovery and downtime
Surgical options require weeks of recovery, anesthesia, and hospital stays. ESG and balloon are outpatient procedures with recovery measured in days. For women managing work, family, or caregiving responsibilities, this is a real difference.
Long-term support
The Everself Program pairs ESG with 12 months of concierge weight care. You get physicians, dietitians, and care coaches supporting you through every stage of recovery and habit change. This kind of structured follow-up is a significant predictor of long-term outcomes.
Risks and What PCOS Patients Need to Know
Every procedure carries risk. Being informed means understanding what you’re weighing.
Surgical risks (sleeve and bypass)
- General anesthesia complications
- Staple-line leaks (sleeve): rare but serious
- Infection, bleeding, blood clots
- GERD worsening (especially with sleeve)
- Nutritional deficiencies requiring lifelong supplementation (especially bypass)
- Irreversibility
ESG risks
ESG has a significantly lower risk profile than surgical options. Reported complication rates are under 2% in large studies. There’s no incision, no general tissue removal, and no permanent anatomical change. Nausea and temporary discomfort in the first few days are the most common side effects.
Balloon risks
Generally mild. Nausea and cramping in the first 1–2 weeks as the body adjusts. Rare risk of balloon deflation or migration, which is why regular follow-up is essential.
For PCOS patients specifically
Pregnancy after bypass requires careful nutritional planning and medical supervision. ESG and balloon carry no comparable malabsorption concern, making them safer options for women who anticipate conception. For many women, starting with non-surgical weight loss procedures offers a lower-risk way to improve metabolic health before considering surgery.
Next Steps for PCOS Weight Loss
PCOS is a manageable condition. With the right support and the right clinical intervention, meaningful weight loss is achievable and it can restore a great deal of what PCOS has disrupted: your cycles, your hormones, your energy, and your fertility.
The best procedure is the one that fits your BMI, your fertility goals, your recovery window, and your long-term plan.
For many PCOS patients, ESG Stomach Tightening® offers that fit: a one-time, non-surgical endoscopic procedure backed by real clinical outcomes, minimal downtime, and the 12-month concierge support of The Everself Program.
Find the weight care plan that fits your goals. Book your consultation today

